Scoliosis, being one of the most prevalent back deformities affecting growing children, with potentially dire consequences, stirs notable anxiety among patients and their families.
There are three common types of scoliosis that affect children [1]
- Idiopathic scoliosis
- Congenital scoliosis
- Neuromuscular scoliosis
Idiopathic scoliosis
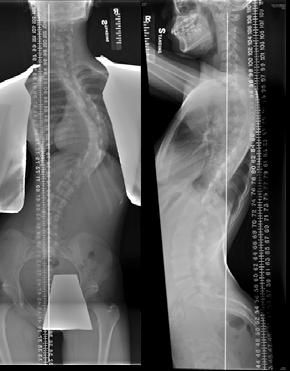
Idiopathic scoliosis accounts for 80-85 % of cases [1]. The spine is normal at birth but develops a deformity in childhood. It can occur in toddlers and young children, but the majority of cases occur from age 10 to 15 (Figs 1 and 2). Two to three percent of adolescents have scoliosis. Boy and girls are equally affected by small curves, but girls are eight times more likely to develop progressive curves. According to recent research, about one in three children whose parents have scoliosis will develop scoliosis. Scoliosis is considered a partially genetic condition. However, exactly which genes cause scoliosis is unknown [2,3]. It’s a common believe that scoliosis cause significant back pain and functional disability. In fact, mild to moderate scoliosis typically does not cause back pain and will not cause compression onto the nerves or the heart and lung. Only very severe scoliosis curves will cause heart and lung problems [1].
|
Fig. 1A Typical right thoracic scoliosis showing a curved back, tilted shoulder, prominent scapula, and trunk listing. |
Fig. 1B Prominent rib hump during Adam's forward bending test. |
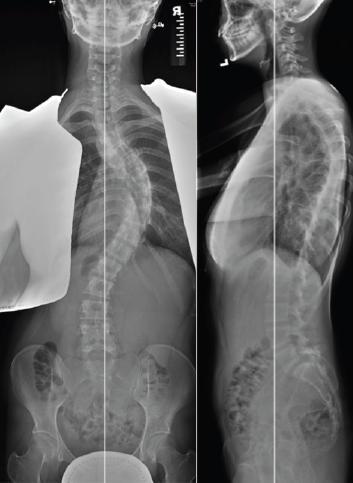
Fig. 2 AP & Lateral radiograph of the same patient. |


Congenital scoliosis
Congenital scoliosis (Fig. 3) starts before birth. Part of one or more vertebrae does not form completely, or the vertebrae do not separate properly. This type of scoliosis can be associated with other health issues, as well as heart and kidney problems [1].
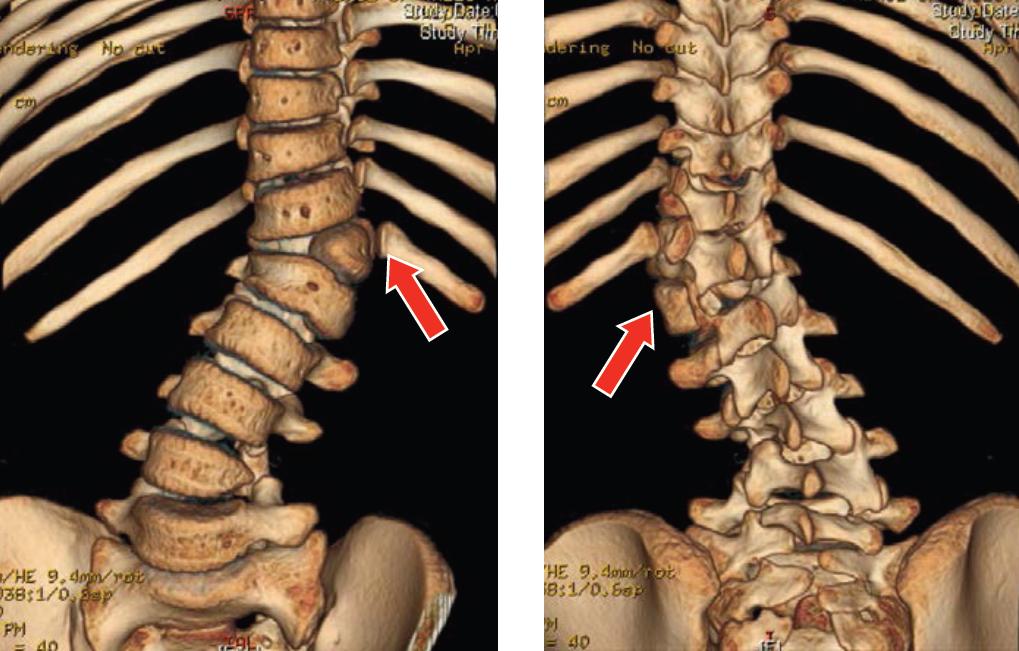
Fig. 3 3D-CT scan of patient with left T12 hemi-vertebra.
Neuromuscular scoliosis
Neuromuscular scoliosis (Figs. 4 & 5) encompasses scoliosis that is secondary to nerve or muscle diseases such as cerebral palsy, spinal cord trauma, muscular dystrophy, spinal muscular atrophy, and spina bifida. This type of scoliosis generally progresses rapidly and often requires surgical treatment.
|
Fig. 4 Severe long thoracic curve in a girl suffering from spinal muscular atrophy. Note significant pelvic obliquity with poor sitting posture. |
Fig. 5 Sitting AP radiograph of the same patient. Note how radiograph shows the true severity of the pelvic obliquity. This is best treated by surgery to allow comfortable seating. |