Pain is a multidimensional experience. Chronic pain differs from acute pain in that it lasts for more than 3-6 months, and there may not be obvious tissue injury leading to the pain. The pathway leading from stimulus to perception may be sensitised [1]. There is often associated depression. Management of chronic pain therefore requires a holistic multi-disciplinary approach [2]. In addition to pharmacological treatment, psychosocial support, physiotherapy and operative treatment, interventional techniques may benefit some patients by defining the pain generator and offers prolonged relief.
Interventional Pain Procedures
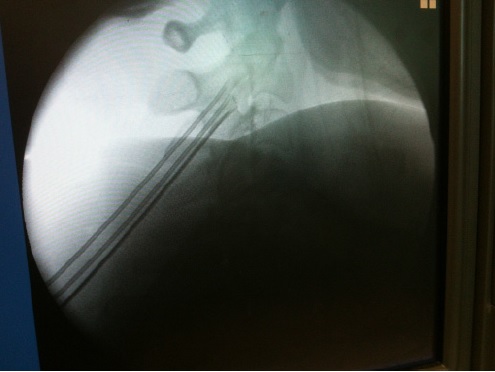
Commonly performed interventional procedures for pain of spinal origin include trigger point injections, facet blocks, sacroiliac joint blocks, epidural steroids and epidural lysis. Blocks with local anaesthetics identify the source of pain when pain level is reduced significantly after the block. Local administration of steroids decreases inflammation. Denervation by a radiofrequency current can bring prolonged relief by interrupting the sensory pathway. A very small group of selected patients benefits from spinal cord stimulation or insertion of an intra-thecal drug delivery system. Diagnostic blocks with a local anaesthetic help to ascertain the source of pain.